
| Status | Physician |
|---|---|
| Country | Papua New Guinea |
Douglas Adrian Russell arrived in Papua New Guinea in 1956 when leprosy was a medically isolated disease. In the next twenty years, he organized an effective leprosy service, undertook epidemiologic, preventative and therapeutic researches and engaged in education campaigns of health workers which laid the foundation for the integration of leprosy into general health services. (205)
Up to 1956, leprosy was considered an increasing problem to be controlled through law and isolation. The leprosy services were limited in money, manpower and direction. This was the situation facing the country’s first time leprologist when he arrived in 1956. (210)
In 1955, the decision to appoint a government leprologist was taken and in November 1956, the country’s first leprologist arrived in Port Moresby.
Douglas Adrian Russell was born in India in May 1918, and graduated MB, BS from Madras University in 1943; from 1946 to 1951, he worked with R S Cochrane, a pre-eminent British leprologist, in Chingleput and Vellore. The next five years were spent at Sungei Buloh Leprosy Settlement in Selangor, Malaysia. He was then appointed to Papua New Guinea:
To formulate, direct and supervise a leprosy control programme, advise on prevention, diagnosis and treatment … to inspect hospitals and leprosaria … to act as consultant specialist to the Department of Health … to prepare reports and articles … and to train staff in the treatment and diagnosis of leprosy.
Apart from some mission doctors, there was little interest in leprosy at the time from the medical establishment. Once he had orientated himself he made four basic observations of fundamental importance to leprosy work:
His first objective was to show that domiciliary treatment of the rural leprosy population was a feasible proposition. In 1958, working with the District medical Officer at Wabag and using the extensive leprosy records of the Yampu leprosarium (a Catholic Institution), he contacted most if not all the leprosy patients in the Wabag District. He then instituted domiciliary treatment through the local health centers and aid-posts and showed that this was accepted by the patients so long as the supply of medicines was within an hour or so walk from the patient’s home.
In the same year with Sister J Phillips (a London Mission Society sister from Cardiff. who had been working in Gemo since 1950), he surveyed the Kerema and Orokolo areas and found a leprosy prevalence of 1.2 per cent of the population. In 1960 with the aid of a grant of 3000 GBP from the Leprosy Mission a leprosy clinic was established at Orokolo for domiciliary treatment. Similair work was also undertaken at Bogia and Begasin. By 1963 Russell estaimated that 80 per cent of the patients in these four schemes were regular attenders. Though the schemes worked well Russell recognized that the training of orderlies, medical assistants, nurses and doctors was inadequate for good leprosy work. The need existed for a separate leprosy service in order to “develop a campaign of control to a level compatible with its eventual absorption into the general health service, by way of the rural health services.”
The Health Department accepted that domiciliary treatment of leprosy patients was feasible and desirable. Russell (1960) could write that “compulsory segregation has been gradually replaced by selective isolation, whereby, as far as possible and practical, non-infectious cases are not sent to leprosaria but are encouraged to receive treatment in their village”. R F R Scragg (1962) stated the health department’s view on this change: “A system of domiciliary care using aid-post orderlies and other medical personnel is being developed in all areas. The response to treatment is excellent …”
By 1967, the scheme had been extended to all major areas of prevalence. The proportion of hospitalized patients and those on domiciliary treatement changed dramatically over the next few years. ….(212)
Russell also appreciated the importance of research and his next major step was to establish a research programme. The role of BCG as a prophylactic for leprosy had been assessed n other parts fo the world with differing methodologies and results. The second report of the Expert Committee on Leprosy of the World Health organization laid down various requirements for accurate assessment of BCG prophylaxis. During 1960, reports from Karimui in what is now Simbu Province indicated that a high prevalence of leprosy existed in the region. As it was known that tuberculosis was rare in the Highlands and that the Karimui people were relatively isolated, it was decided to undertake a trial of BCG in this population. Russell visited Karimui in February 1961 and in a pilot survey confirmed the high prevalence of leprosy in the area (68 cases among 1114 persons examined, a prevalence of 6-1 per cent). …
In 1962, the first full population census was taken: to facilitate this task, Russell offered an axe to the first village leader who presented a complete line up of his village. When his promise was made good on the fifth day he had no further problems of attendance. A survey showed a leprosy prevalence of 5.9 per cent of 5063 persons of all ages examined. In the trial, 2318 persons were given BCG, and 2295 received saline injections. The details of the trial methodology have been described by Russell, Scott and Wigley (1964). Extensive resurveys were subsequently carried out, with remarkable re-attendance rates; Russell attributes this success to the excellent public relations which were established with the Karimui people. … in brief, by 1967, eight leprosy cases were found in the vaccinated subjects compared to eighteen in the control subjects. The maximum protection was achieved in the 10-29 year age group, but in persons over 30 years and children under 10 years no significant differences were noted. Since the prevalence of lepromatous cases was always low, it was not possible to determine the protective effect (if any) of BCG against this form of the disease; the maximum protection was recorded against the borderline-tuberculoid (BT) form of the disease. During this period, because of the isolation of the people, no regular treatment had been given to the patients. In 1967, the depot sulphone DADDS (diacetyl derivative of diamino diphenyl sulphone) became available: it was felt to be ethically unjustified to withhold treatment and in November 1967 injections of DADDS were given to all known available patients every 75 days. …. (213)
The treatment was welcomed by the patients, health personnel and village councilors who soon realized that early and effective treatment was associated with a decreased incidence of deformity and visible stigma of leprosy. D R Vincin (a European Medical Assitant who headed the Highlands Regional Leprosy Control Unit) writes that “the population in general have endorsed this drug programme on the considered improvement of patients in their midst and are enthusiastic on its continuance, naturally hoping for the eradication of the disease from the area”. Unfortunately, the DADDS program has petered out from all areas except Karimui.
A number of genetic and immunological studies were carried out in Karimui. …
Russell’s brief included a commitment to “formulate, direct and supervise a leprosy control programme”. Because of the rurality of the disease, and the difficulty of the terrain, he felt that specific surveys for leprosy case-finding would be the most efficient form of control. To this end he developed Regional Control Units whose function would be to maintain leprosy registers, control the discharge of patients from leprosaria, maintain and supervise treatment programs, particularly domiciliary programs, carry out health education and undertake case-finding surveys.
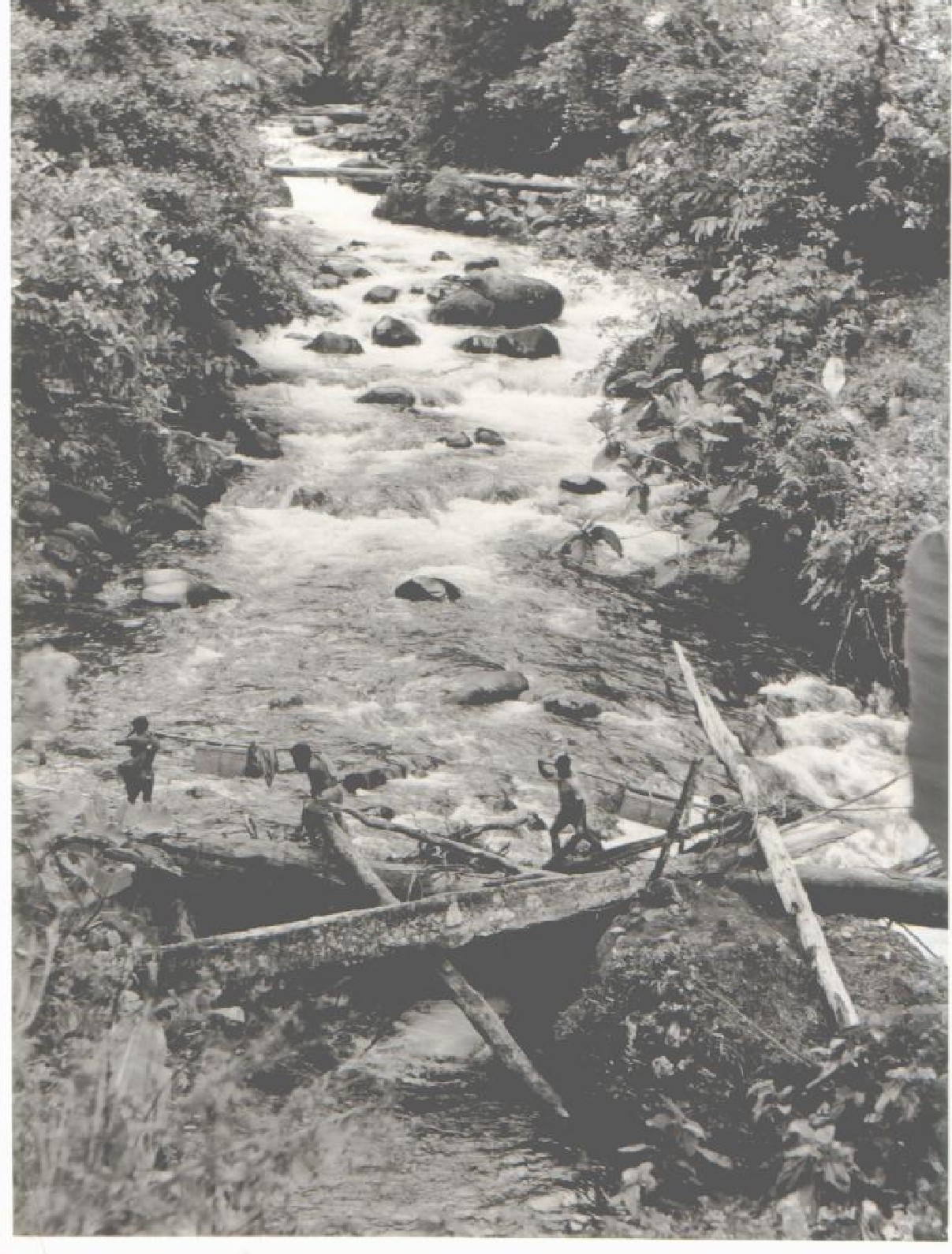
Crossing a bridge, while on patrol in the PNG Highlands (From the Personal Collection of Dr D A Russell)The first unit was the Highlands Regional Leprosy Control Unit, established in 1963 at Moutn Hagen under the direction of R Rodrigue. Subsequently, further untis were established at Rabaul (New Guinea islands Region, 1964), Port Moresby (Papuan Region, 1964), Mandang (Mainland, 1965) and Maprik (East and West Sepik, 1970). Because of the lack of interest in leprosy work by the medical establishment, much of the work of the units was controlled by medical assistants. The regional units were at all times under the direct control of Russell and represented the paradigm of vertical control. In addition to these administration units, a unit was established by the Leprosy Mission in 1967 at Tari, in the Southern Highlands, originally for reconstructive surgery but later supervising all the leprosy work in the area including survey programs and health education.
The regional units rapidly established themselves as effective units. Extensive case detection surveys were undertaken. In 1967-70 over 240 000 people were examined for leprosy with 575 new cases of leprosy detected. In the Highlands alone, between 1963 and June 1974, 9500 leprosy patients were registered. … (214)
With the advent of suphones, it was felt that the effective treatment of the maximum number of infectious patients must ultimately produce a reduction in the incidence of the disease to a point where transmission would cease. Case-finding followed by effective chemotherapy should in practice do what segregation has done a century previously in other countries. The scientific basis for this belief has not in fact been established and thee is some evidence that infectious leprosy patients can be shedding M Leprae from the nose before skin or neurological changes are evident. The Karimui DADDS trials did show, however a very significant decrease in the incidence of new cases of leprosy in Karimui. … (215)
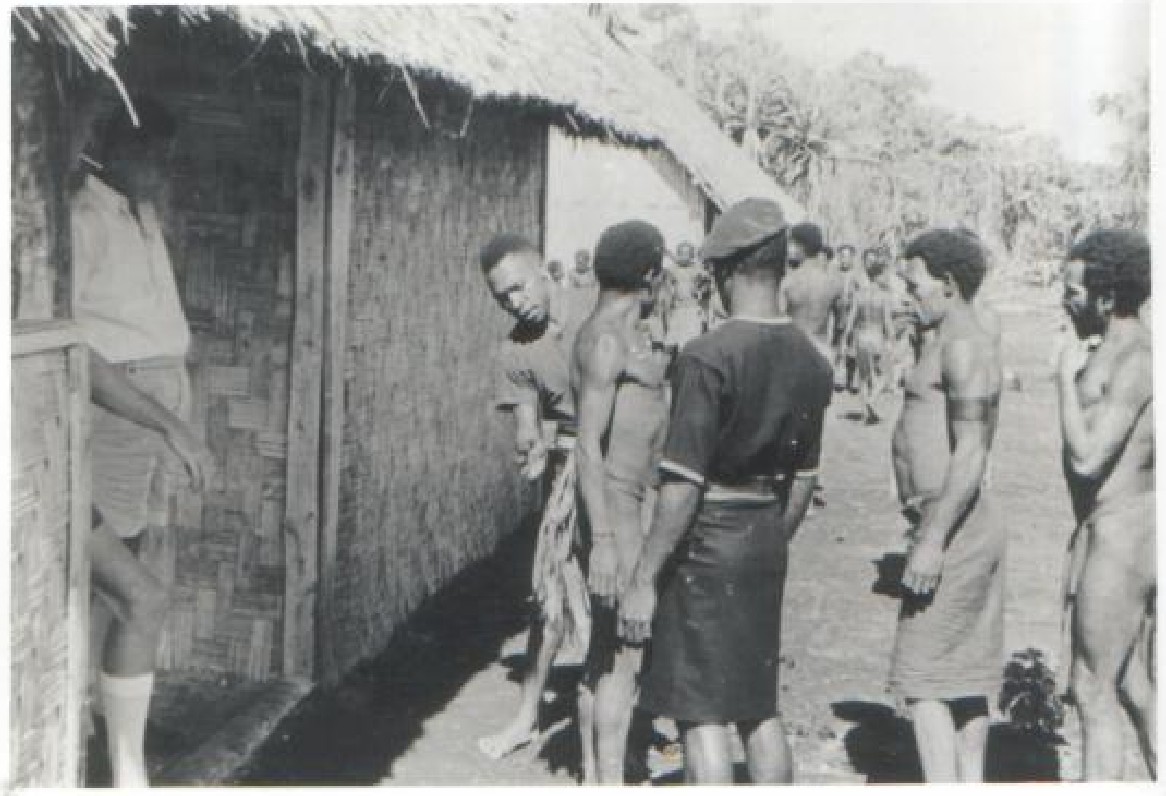
First visit and sample survey at Karimui Patrol Post (From the Personal Collection of Dr D A Russell)The final step Russell took was to start the process of integration. He had always believed in integration though recognizing the need for a separate leprosy service in the early stages of leprosy control. His early domiciliary treatment trials demonstrated that integration was feasible. In March 1970 the Public Health Department created a Division of Community health which comprised essentially the field services of the department … The central objective of the division was to develop a community health service at the district level. The basis for this service would be the rural health center which should be able to provide a complete health service to the community including the provision of special clinics for leprosy. Following this political change Russell presented a paper at the District Health Officer’s Conference in November 1971 which stated that
The professional and technical aspects of the leprosy control programme are subject to central direction and control from the Senior Specialist Medical Officer (Leprosy) with District Health Officers being responsible for carrying out the planning, programming, organization, conduct and supervision of leprosy control measures within districts according to central policy.
From now on the Health Department would state the objectives of the leprosy program, but the Districts would put the program into effect: this was reiterated in the National Health Plan 1974-78 in which it was stated that “the management and control of leprosy is a function of the general health services and the responsibility of the district health officers.”
The regional control units worked from 1972 in close collaboration with District Health Officers until their disbandment in October 1973. In that month, A Toua, the Director of Public Health, confirmed that District Leprosy Control Programs would be the norm from then on.
In September 1973 J C Tao, the WHO Adviser on Tuberculosis, visited Port Moresby and advocated a joint tuberculosis/leprosy headquarters unit. In May 1974 Russell and K Wari, who had taken over the Tuberculosis Programme from S Wigley, set up a combined office in Konedobu. He was assisted by three medical assistants.
Cocurently, localization of the leprosy program was proceeding apace. By 1975, of the seventeen districts then in existence, six were headed by national officers, mainly Health Extension Officers (HEOs) and hospital assistants and this number was soon to increase. … (216)
Reconstructive surgery of leprosy patients in Papua New Guinea started in 1965. The impetus for this, once again, originated with Russell. … By 1963, he estimated that 2200 leprosy patients out of a total of “about” 10 000 cases in the country were in need of specialized surgical assistance. Two major problems presented themselves: firstly, leprosy in PNG is not associated with the social ostracism seen in some countries; the pressure for cosmetic care does not therefore exist. Secondly, the leprosaria, caring for the great majority of leprosy patients, were generally sited far from general hospitals and were largely unsuitable for surgical work. Despite these constraints, Russell, while attending the International Congress of Leprosy in Rio de Janeiro in 1963, persuaded Brand to accept a trainee for reconstructive surgery…. (218) In November 1963 Russell offered the post to Dr J K A Clezy, at the time Specialist Surgeon in Rabaul. … (218)
Russell was fortunate to arrive in PNG at a time of worldwide increasing interest in leprosy and PNG was fortunate to appoint a leprologist of great skill and determination whose impact on the disease has been immense. Her contribution may be briefly summarized:
Russell left PNG on 8 November 1976 after twenty years of impressive work: the leprosaria were closed or closing; leprosy control though still under central direction was firmly in the hands of provincial health officers and their leprosy control officers – by now mainly locally trained health extension officers or nurses. The standard management of leprosy in PNG has been described by Myra Kennedy (1979). Headquarters formulates policy but it is carried out largely by general health workers. Provincial leprosy control officers exist to explain and teach the program to all health workers and to provide expertise in the management of patients. The following pointers indicate the degree of integration which has occurred:
(Extracted from G H Ree "Leprosy - the Development of an Integrated Service" Chapter 9, 205-229) in A History of Medicine in Papua New Guinea, ed Sir Burton G Burton-Bradley, Australasian Medical Publishing Co, 1990.)
Treatment Used/Researched:
Reconstructive Surgery
Russell DA, "Notes on Leprosy in the Territory of Papua New Guinea," IJL, 27(1958) : 26-30.
----, "Leprosy in Papua New Guinea," PNG Med J 4 (1960): 49-54.
----, "Case-Finding, Follow-up and Management of Leprosy Cases with Particular Reference to the Integration of these Activities into those of the Established Health Services," WHO Technical Discussions, WP/RC 14/TD6, 1963, 11 pages.
----, "Leprosy in the Territory of Papua New Guinea," South Pacific Bull, 17 (1967): 31-4.
----, "Leprosy (including Administration) in the Territory of Papua New Guinea," (Abstract) IJL 36 (1968): 603.
----, "BCG Vaccination in the Prophylaxis of Leprosy," 10th International Leprosy Congress, Bergen 1973 (Abstracts), 7 (1973): 221: 135.
----, "Leprosy in Papua New Guinea," PNG Med J (1973): 83-5.
----, "The Treatment of Leprosy in Papua New Guinea," PNG Med J 16 (1973): 124-6.
----, "Leprosy Control", Public Health Department, Port Moresby, mimeographed paper, 9 pages.
Russell, DA and Bell CO "Leprosy in the Diseases and Health Services of Papua New Guinea 1974-1978," ed C O Bell, Public Health Department, Port Moresby.
Russell, DA, Peters JH, Vincin DR, Scott GC and Shepard CC, "Clinical Assessment at Five Years in the Acedapsone (DADDS) Trial in the Karimui, New Guinea: Correlation with Plasma Sulphone Levels," 10th International Leprosy Congress, Bergen, 1973 (Abstracts), 2 (1973): 6:4.
Russell, DA, Price MA, Anders RF, Anders EM and Goldring ES, "Cell-Mediated Immunological Status of Leprosy Free Members of Families with a History of Lepromatous Leprosy," 10th International Leprosy Congress, Bergen, 1973 (Abstracts), 12 (1973): 96:61.
Russell, DA, Scott GC, "A Preliminiary Report of a `Blind' Control Experiment in Investigations on the Effect of BCG Vaccination on Leprosy in a Closed Community," 10th International Leprosy Congress, Rio de Janeiro, 1963.
Russell DA, Scott GC, Vincin DR and Boughton CR, "The `Flare' Phenomenon and the Use of `Hansolar' (Acedapsone, DADDS) in the Control of Leprosy," In: 10th South East Asian Regional Seminar on Chemotherapy in Tropical Medicine, Bangkok, (Abstracts) 1971.
Russell, DA, Scott GC and Wigley SC, "BCG Vaccination in Leprosy: a Preliminary Report of `Blind' Controlled Trials", IJL, 32 (1964): 235-47.
----, "BCG and Prophylaxis - the Karimui Trial" (Abstracts), IJL 36 (1968): 618
Russell, DA, Shepard, CC, McRae, DH, Scott, GC and Vincin, DR, "Treatment with 4, 4-diacetyldiamino-diphenyl sulphone (DADDS) of Leprosy Patients in Karimui, New Guniea", Am J Trop Med Hyg 20 (1971): 495-501.
----, "Acedapsone (DADDS) Treatment of Leprosy Patients in the Karimui of Papua New Guinea: Status at Six Years," Am J Trop Med Hyg 24 (1975): 485-95.
Russell, DA, Shepard, CC, McRae, DH, and Vincin, DR, "Present Status in the Acedapsone Therapeutic Trial in the Karimui, and its Relationship to Other Trials," IJL 42 (1974): 125-6.
----, "Prevention of Leprosy by Acedapsone," Lancet 2 (1975): 771.
Scott, G C, Wigley S C and Russell D A, ""The Karimui Trial of BCG 2: Tuberculin Reaction in a Leprosy Endemic but Tuberculosis Free Population," IJL 34 (1966): 139-46.
----, "The Epidemiology of Leprosy - the Karimui Trial," In: 9th International Leprosy Congress, London (Abstract), 11 (1968): 4.3.
Russell, DA, Vincin, DR, Shepard, CC "Status at Ten Years of the Leprosy Patients in the Acedapsone (DADDS) Trials in the Karimui, New Guinea," 11th International Leprosy Congress, Mexico City, 13-18 November 1978, (Abstracts) 123.
Russell, DA, Wigley, Vincin, DR, Scott, GC, Booth, PB and Simmons RT, "Blood Groups and Slivary ABH Secretion of Inhabitants of the Karimui Plateau and Adjoining Areas of the New Guinea Highlands", Human Biology in Oceania, 1 (1971): 79.
Russell DA and Wigley SC, "Leprosy and Tuberculosis", Encyclopaedia of Papua and New Guinea 2 (1972): 640.
Stanhope JM, Sturt RJ and Russell DA, "An Outbreak of Leprosy in a Previously Unexposed Population of Eastern New Guinea", Transactions of the Royal Society of Tropical Medicine and Hygiene 62 (1968): 700.
Russell DA, Vincin DR, Boughton CR, and Scott GC, "The Karimui Study. The Role of the Case-Finding and Treatment with Regard to the Prevention of Disability and Deformity in Leprosy", Proceedings. Review Twelfth World Congress on Rehabilitation International Sydney, Australia. 2 (1972): 233.
Russell DA, Clezy JKA, Price, MA, Kennedy M, and Taylor, V, Handbook for Leprosy in Papua New Guinea, Department of Public Health of Papua New Guinea, 1974.
Bagshawe, A, Scott, GC, Russell DA, Wigley, SC, Merianos, A and Berry G, "BCG Vaccination in Leprosy. Final Results of the Trial in Karimui Papua New Guinea 1963-79", Bulletin of the World Health Organisation 67.4 (1989): 389-99.
Russell, Doug, MBBS. DPH. FRACMA. "Leprosy: Its Salient Features and Recommended Therapy" Australian Family Physician. Journal of the Royal Australian College of General Practitioners, 16.2 (February 1987).
Shields, ED, Decary, F, Russell, DA, "Genetic Distance: Probing the Origin of a Papua New Guinea Isolate", International Journal of Anthropology 1.4 (1986): 307-22.
Shields, Edward D, Russell, Douglas, and Perikak Vance, Margaret A,"Genetic Epidemiology of the Susceptibility of Leprosy", J of Clinical Investigation. The American Society for Clinical Investigation 79 (April 1987): 1139-1143
Cochrane, RG, Ramanujam, K, Paul, H, Russell, D, "Two and a Half Years Experimental Work on the Sulphone Group of Drugs", Leprosy Review 20 (1949): 4.
"Recommendations made Following the Visit to China (Taiwan). 6 August - 10 September 1968 and 24 September - 10 November 1968" by Dr DA Russell. WHO Short-Term Consultant on Leprosy .
Hale, JH, Molesworth, BD, Grove-White, RJ, Sambamurthi, CM and Russell DA, "The Relationship and Significance of the Mantoux and Lepromin Reactions in Leprosy", IJL 23 (1955): 139-47.
"Leprosy Update", Paper presented at Australian Society for Microbiology. Brisbane Conference, Public Health Plenary Session, Tuesday 7th May 1983.
Hale, JH, Molesworth, BD, Russell, DA, Lee JH, "Isonicotenic Hydrazide in the Treatment of Leprosy" IJL 22 (1954).
Russell, DA, Worth RM, Scott GC, Vincin, DR, Jano, B, Fasal P, and Shepard, CC, "Experience with Acedapsone (DADDS) in the Therapeutic Trial in New Guinea and the Chemoprophylactic Trial in Micronesia", IJL 44: 1 and 2 (1976): 170-76.
Peters, JH, Murray, JF, Gordon, GR, Levy L, Russell, DA, Scott, GC, Vincin, DR, and Shepard CC, "Acedapsone Treatment of Leprosy Patients. Response Versus Drug Disposition", The American Journal of Tropical Medicine and Hygiene 26 (1977): 127-135.
Russell, DA , Worth, RM, Jano, B, Fasal, P and Shepard, CC, "Acedapsone in the Prevention of Leprosy: Field Trial in Three High Prevalence Villages in Micronesia", Am J Trop Med Hyg 128.3 (1979): 559-63.
Shields, FD, Russell, DA, Vincin, DR, Scott, GC, Abstracts, Paper 8 11th International Leprosy Congress, Mexico City, 13-18 November 1978.
McAdam, KP, Anders RF, Smith SR, Russell, DA, and Price, MA, "Association of Amyloidosis with Erythema Nodosum Leprosum Reactions and Recurrent Neutrophil Leucocytosis in Leprosy", Lancet 2.7935 (1975): 572-3.
{kind=link}
{kind=link}