


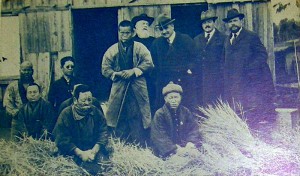
Staff of Tama Zensho-en (Zensei Hospital)
At the turn of the twentieth century, when it appeared that Japan had an inordinately large number of leprosy sufferers, it was considered a national disgrace. Dr Kensuke Mitsuda (1876-1964), who was the most influential leprologist in the country, lamented the representational impact of the statistics: “Japan, a country proud of the purity of its own pedigree and blood, is now known as the world’s leading leprosy nation, far worse than European and American nations.” He was deeply concerned that the nation would be considered “barbarous, uncivilized and primitive”. (Japan Law Foundation, p. 121)
Subsequently, in 1907, what is now known as the (Old) Leprosy Prevention Law was enacted, having application mainly to vagrants affected by the disease. As part of this initiative, the country was divided into five regions and a public sanatorium was established in each region. After World War I, the new public health policy moved more strongly towards ensuring absolute segregation by expanding sanatoria and, among other measures, providing abortion “when requested by a patient”. In addition the revision of the (Old) Leprosy Prevention Law gave superintendents the authority to discipline inmates, adding a dimension of criminality to leprosy confinement in Japan. This was intensified with the use of cells to imprison recalcitrant inmates or those who had been convicted of a crime.
Leprosarium in Shizuoka
An expansion programme began with the purpose of establishing a system of state-run sanatoria in 1927 and a mega colony like Culion, in the Philippines, called Nagashima Aiseien, Okayama, was conceived on an island in the Inland Sea. (Ohtani, 70) In 1931 the (Old) Leprosy Prevention Law was widened in scope to apply to everyone suffering from leprosy, rather than those who were vagrant and this legislation was accompanied by the establishment of a national or state run system of sanatoria. This widened version of The Leprosy Prevention Law was established immediately before the fifteen year period of war in which Japan fought in Asia and the Pacific: “In the midst of this prolonged war period, the policy on Hansen’s Disease was also placed within the framework of a eugenic policy to create better citizens who were superior physically and psychologically.” (Japan Law Foundation, p. 23)
Hence the prefectures were able to rid themselves of people with the disease through the Leprosy Free Prefectures Campaign which entailed removal of all leprosy-affected people into sanatoria. (Ohtani, p. 63)
Then in 1948 the Eugenic Protection Law legalised sterilization and the termination of pregnancies. *2 After the war, the government continued its policy of increasing admissions and accommodation within the sanatoria, admitting 4,500 in 1949. The committee found that “After the war was lost, the idea of enhancing the eugenic policy to build a “civilized nation” was very strong among the population policy makers and doctors at the time.” (Japan Law Foundation, 54)
While these laws were obviously draconian and had a profound impact on the lives of people suffering from leprosy, they did not incur international censure at the time. In fact, international and national policies on leprosy elsewhere parallel those formulated in Japan up until the 1950s. The (Old) Leprosy Prevention Law of 1907 was in concert with the Berlin and Bergen International Leprosy Conferences of 1897 and 1909 which recommended segregation. The establishment of national leprosaria in Japan coincided with the building of leprosy colonies and the enactment of legislation in other parts of the world. *3 This was the period of the “model” leprosy colony or settlement influenced by Molokai, Hawaii and the Culion Leper Colony and the hospital and agricultural colony of Fontilles in Spain that was established in 1907.*4

Dr. H. W. Wade (centre) with Drs K. Yamamoto, S. Nakajo, K. Kusama, and other Japanese health officials and asylum directors.
Additionally, Japan’s policy on leprosy was continually reported internationally without adverse comment and was in fact considered praiseworthy. Leprosy in India in 1935 contained notes from a journey to Japan by Dr Isaac Santra. He reported that “every patient on death is autopsied” and there was a “vast collection of material” at Aiseien Nagashima, Okayama. He also learnt that the married male patients were sterilised on their own consent. Santra, Leprosy in India) He described how at Oshima, since 1909, 600 cases had died and the viscera of 230 had been preserved in 10% formalin. He was also aware that autopsies were being performed on foetuses, as well, because he stated that M. leprae had been found in the viscera of the foetus but they were difficult to differentiate from the tubercle bacillus.
One of the significant differences between Japan and the rest of the world at this stage was the refusal to see sterilisation within the context of eugenics. At the inaugural “All India Leprosy Workers Conference” in Wardha, India, in 1948, Dr Dharmendra presented a paper on the place of sterilisation and particularly vasectomy in leprosy control arguing that although it could not be considered on eugenic grounds because there was no evidence that it had a familial basis, it had a place principally in infective or suitable cases, provided it was on a voluntary basis, in order to prevent the spread of the disease. (Dharmendra) He drew heavily on the example of Japan and cited a considerable body of literature from Japanese studies explaining their national policy, the matter of consent, its negligible impact on the sex drive and also on the progress of the disease, as well as its function in preventing pregnancies which were considered to exacerbate the disease. He then outlined a proposal for sterilisation in India. This proposal listed likely candidates such as couples in institutions who wished to pursue married life, those who committed crimes of a sexual nature, and those living in informal or self-settled leprosy camps and bustees where children may be exposed to the disease. (Dharmendra, p. 69) He argued that the most common ground for sterilisation in cases of leprosy is the prevention of the spread of the disease by preventing the birth of children who would be exposed to leprosy. (“Social and Economic Aspects of Leprosy”, p. 29) The following discussion was quite divided and was summed up by the Chairman as being about a highly controversial topic, but everyone was in agreement that there should be no vasectomy on a compulsory basis. (Social and Economic Aspects of Leprosy, p. 31) The issue of consent made all the difference to the acceptance of sterilisation. It became clear long afterwards that although the doctors in Japan seemed to believe that consent had been obtained and in fact assured their overseas medical visitors, many, many people who were sterilised would later reveal that they really didn’t have a choice.
Finally in 1953, the (New) Leprosy Prevention Law was enacted and by 1955, 91 percent of all leprosy-affected people in Japan were isolated. Although Robert Hastings, the American editor of the International Journal of Leprosy, points out that this (New) Leprosy Prevention Law differed little from laws in various states of the United States at that time, while legislation was still in existence in most parts of the world, this new Japanese legislation was enacted at a time when leprosy institutions throughout the world were opening their doors and discharging their inmates. The new drugs promin and dapsone were making a dramatic difference to the symptoms of leprosy, and people who had been isolated from society for years were struggling to re-enter the outside world. A WHO study on legislation published in 1952 stated that “At the present time, the compulsory isolation of lepers [sic] is still the most commonly employed method of control in use in those countries where leprosy is endemic. Doubt has been thrown on the efficiency of this method by the observation that leprosy has not always diminished where such a policy was vigorously applied … It is for this reason that the Committee recommended that “only infectious cases need to be subjected to some form of isolation” …(WHO Review of Legislation)
Nonetheless the standard medical textbook by Sir Leonard Rogers and Ernest Muir that was published in its third edition on 1946 was still in concert with the Japanese approach. It stated that sterilisation was a viable option in “backward countries” (ironically, the very designation that Japan had sought to avoid by instituting such thorough and uncompromising efforts against the leprosy-affected):
Owing to difficulties in backward tropical countries in the safe separation of infants from their leper parents early enough to prevent the possibility of their infection, the most effective methods of preventing married patients from begetting children is by sterilization. … the marriage of lepers in institutions should only be permitted subject to the same operation being first performed, as has been done by the Americans in Panama. Such expedients are only required when the circumstances do not permit of the strict enforcement of the general rule to isolate the sexes completely in leper settlements. (Rogers and Muir)
Throughout the world, administrators were caught by the isolation system. They either had to segregate the sexes for the lifetime of the inhabitants; or face the fact that their colonies were breeding grounds for children who were candidates for the next generation of leprosy-affected sufferers; or they had to sterilize their inmates, having first “obtained consent”. Whatever they did, they were unable absolutely to prevent unwanted births. One Japanese woman’s experience explains what happened when she was discovered to be seven months pregnant. Having been strongly advised to undergo an abortion, she remembers the child moving its hands and legs on the operating table and the nurse covering the nose and mouth of the baby to stop it from breathing and saying to her “it is a cute girl and looks very like you.” (Miyasaka, p 3) The poetry of Haruko Tsuda who was isolated at eighteen and died in 1963, in 1961 expresses the grief of the people who were subject to these policies:
Collection of literary works by leprosy-affected people
Lying amidst the tattered dark blue bedclothes
I feel like a convict
Not permitted to give life
In the twilight years of life
No child to muse about
Time passes slowly
When waiting for death
While not one familiar face comes to call
In many ways, the public health response to leprosy in Japan represented an intensification of responses elsewhere.
At the Kumamoto District court hearing in 2001, the judge ruled that the Leprosy Prevention Law of 1953 was unconstitutional because it had gone well beyond what was a reasonable restriction for the sake of public welfare, to the extent that its unconstitutionality was already well known. (Japan Law Foundation p. 9) The government decided not to contest their case and subsequently commissioned an investigation into the segregation policy that had resulted in the violations of the human rights of the people so confined. The sum of 1.8 billion yen (₤10.4 million) was awarded to 127 former leprosy patients in compensation for their experiences. (Gould p. 374)
In 2005, in a first for the world, the Japanese government would appoint a committee to investigate the impact of the segregation policy on leprosy-affected people in Japan. This would result from a legal challenge mounted by surviving residents of Japanese sanatoria against their government for the treatment they had experienced.
*1 In 1900 there were 30,359 leprosy-affected people in Japan and in 1923, there were 100,000 reportedly affected by the disease. Susan Burns discusses the shame that these figures represented as well as the collapse of the distinction between actual sufferers and those who were in the same familial “lineage” as those with the disease. pp. 108-9.
*2 Ohtani states that “nearly all of those who reside on state-operated sanatoria have been surgically sterilized.” p. 37.
*3 In Nigeria, in March 1908, a Lepers’ Ordinance was passed for the Colony of Southern Nigeria.
In 1905, legislation was put into place authorising the creation of the Culion Leper Colony Reservation.
The United States of America with the provocation of John Early, a leprosy-affected veteran of the American-Spanish war, and the support of William Danner from the American Mission to Lepers, enacted legislation in 1917 to create a national leprosarium.
*4 J Bernabeu-Mestre and T Ballester-Artigues Bernabeu-Mestre J and Ballester-Artigues T “Disease as a Metaphorical Resource: The Fontilles Philanthropic Initiative in the Fight against Leprosy 1901–1932”, Social History of Medicine 17/3 (2004): 409–421.
Sources
Susan Burns, From “Leper Villages” to Leprosaria: Public Health, Nationalism and the Culture of Exclusion in Japan” in Carolyn Strange and Alison Bashford (eds), Isolation: Places and Practices of Exclusion (London and New York: Routledge, 2003), pp. 104-18.
—, “Making Illness into Identity: Writing” Leprosy Literature” in Modern Japan.” Nichibunken Japan Review (2004): 191-211.
—, “Rethinking ‘Leprosy Prevention’: Entrepreneurial Doctors, Popular Journalism, and the Civic Origins of Biopolitics.” The Journal of Japanese Studies 38.2 (2012): 297-323.
Section V “Social and Economic Aspects of Leprosy” and Dr Dharmendra, “The Place of Vasectomy in Leprosy Control”, Leprosy in India, Special Issue: All India Leprosy Conference, Wardha 20.1 (1948): 28-31 and 63-75 respectively.
Tony Gould, Don’t Fence Me In: From Curse to Cure: Leprosy in Modern Times (London: Bloomsbury, 2005), p. 374.
Japan Law Foundation, Verification Committee Concerning Hansen’s Disease Problem.
Michio Miyasaka: ‘Punishing Paternalism: An Ethical Analysis of Japan’s Leprosy Control Policy’, Eubios Journal of Asian and International Bioethics, 19 (4), 103-107, 2009
Fujio Ohtani, The Walls Crumble: The Emancipation of Persons Affected by Hansen’s Disease in Japan (Tokyo: Tofu Kyokai Association, 1998)
Sir Leonard Rogers and Ernest Muir, Leprosy 3rd edition (Bristol, 1946).
Dr Isaac Santra, “Notes on Leprosy in Japan,” Leprosy in India (1953): 26-7.
Santra ended his report saying that “Places of isolation are not isolated places in Japan. The leper [sic] is happy and active… All the conveniences of the West are combined with the hospitality of the East.” The doctors very generously shared their work with him saying that “Nothing is secret in Japan except the military.” p. 28
Haruko Tsuda Cited
World Health Organisation, Leprosy: A Survey of Recent Legislation (Geneva: WHO, 1954) reprint from the International Digest of Health Legislation 5 (1954).