
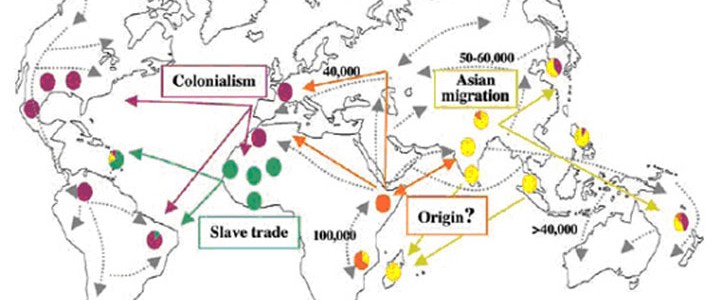
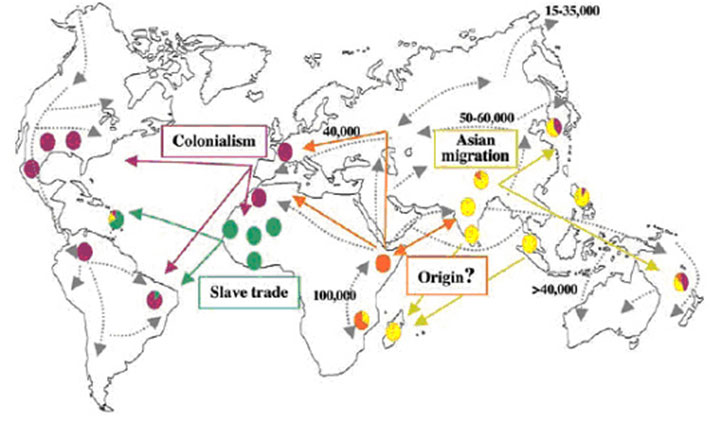
Recent archaeological findings of the skeletal remains of a middle-aged male from the second millennium BC showing the changes characteristic of leprosy have been identified in Rajasthan, India. This evidence demonstrates that leprosy existed in this region at least 4,000 years ago, having spread along trade routes between East Africa and northern India. Genome studies are currently hoping to determine how this strain of M. leprae fits with those that have already been traced (Live Science).
In India, ancient Hindu sources dating from 600BC, the Charaka Samhita and the Sushruta Samhita refer to leprosy under the names “vata-rakta”, “vata-shonita” and “kushtha”. The Sanskrit word “kustha” refers to skin diseases in general. The disease was considered to be both hereditary and highly contagious, communicated through sexual intercourse, touch, breath, or sharing bedding or food. It was also believed to come about through divine retribution. Assisted suicide was a viable option for sufferers. Before the advent of the British in India, people affected with leprosy were often the subjects of benevolence and found shelter in charitable establishments (Wilson).
This region has a quarter of the world’s population and the most new cases of leprosy still occur in this region every year. The countries in the WHO South-East Asia region are Bangladesh, Bhutan, Democratic People’s Republic of Korea, India, Indonesia, Maldives, Myanmar, Nepal, Sri Lanka, Thailand, and Timor-Leste.
The response to leprosy in the eighteenth and nineteenth century in this region is part of the history of colonialism. This is nicely described in Rita Smith Kipp’s “The Evangelical Uses of Leprosy”, Social Science and Medicine 39.2 (1994): 166-178.
Abstract: The history of leprosy treatment among the Karo of Sumatra illustrates how leprosy afforded missionaries an evangelistic opportunity, and how that opportunity eroded in the twentieth century with changing therapies for the illness. Because it symbolized Christian charity, leprosy care drew donations and support for the missionary movement of the nineteenth century. In Karoland, as elsewhere, leprosy patients were attracted to the missionaries’ religion because therapy entailed separation from kin and community and then incorporation into a new kind of community, an asylum, where the authority structure, the dispensation of resources, and the constructed spaces of everyday life made the idea of a supreme deity an experienced reality. When therapies of leprosy shifted to an out-patient system, one of the older missionaries to the Karo struggled to maintain control of the leprosarium that had been one of the few pockets of conversion in this mission field.
Missionary work against leprosy was widespread in this region. The Leprosy Mission had been active from the 1870s. Wellesley Bailey, an Irish missionary with the Church of Scotland, became aware of the plight of people with leprosy, in India, in 1869, in Ambala, in the Punjab. His letters inspired three Dublin friends, the Misses Pim, to organise small meetings in order to support him. The success of their appeals set the foundation for the Mission to Lepers in India, which established its own leprosy asylums and supported those of other missionary organisations. Today the Leprosy Mission still supports leprosy work throughout the world. With the introduction of the sulphone drugs and the beginning of international health coordination, the influence of the missionary organisations changed. As they secularised and professionalised, they began to work with national organisations to coordinate public health approaches to the disease.
By 1987, all endemic countries had begun implementing of MDT, but coverage varied from seventy-one per cent in Thailand to nine per cent in India (Implementation Meeting). Of the more than eleven million estimated leprosy cases in the world, 5.36 million were from the countries of South-East Asia, where leprosy continued to be an important health problem in nine of the eleven countries of the region (Jakarta Meeting). MDT use gradually became widespread and this significantly reduced the disease burden in the region. Yet even by 2013, the problem of leprosy remained for some countries (Leprosy Summit Bangkok).
Dharmendra, “Leprosy in Ancient Hindu Medicine”, Leprosy in India 12.1 (1940):19-21.
International Leprosy Summit, titled “Overcoming the remaining challenges” held in Bangkok, Thailand, 24–26 July 2013.
Smith Kipp, Rita. “The Evangelical Uses of Leprosy.” Social Science & Medicine 39.2 (1994): 165-78.
Live Science Staff, “Earliest Known Case of Leprosy Unearthed”, Live Science May 26 2009. http://www.livescience.com/5456-earliest-case-leprosy-unearthed.html
National Leprosy Consultative Meeting, Jakarta, Indonesia, “Leprosy Profile in South-East Asia Region Countries” Nov 28-Dec 3 1988 [Leprosy: Group Consultations and Training Activities – General L4/48/1 vol 1 no 1], p. 1
S S Pandya, “Very Savage Rites”: Suicide and the Leprosy Sufferer in Nineteenth Century India. Indian Journal of Leprosy 73 (2001), 27-38.
“Report of the Second Coordinating Meeting on Implementation of Multidrug Therapy in Leprosy Control Programmes” Geneva 4-5 Nov 1987, p. 20 [WHO/CDS/LEP/87.2]
H H Wilson, “Kushta, or Leprosy”, Transactions of the Medical and Physical Society of Calcutta 1 (1825): 1-44.